J.ophthalmol.(Ukraine).2016;3:41-45.
|
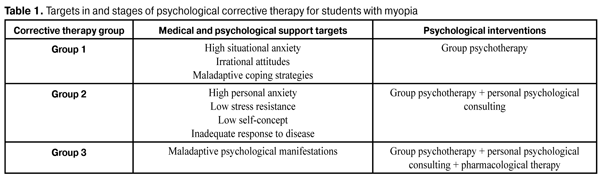
https://doi.org/10.31288/oftalmolzh201634145 Monitoring of psychoemotional status in myopes after psychological correction of maladaptive individual psychological features N.A. Ulyanova1, Dr Sc (Med) K.V. Aymedov2, Dr Sc (Med), Prof. N.S. Semeniuk, MD 1Department of Ophthalmology, Odessa National Medical University 2Department of Psychiatry, Addiction, Psychological and Social Assistance, Odessa National Medical University Odessa, Ukraine E-mail: ulyanova@ukr.net Background: Progression of myopia in a pediatric or adolescent patient is asymmetric, with periods of rapid increase in axial (anteroposterior) length (and, consequently, in refraction) coinciding with periods of significant increase in anthropometric measurements. Previously, we have found an association between psychoemotional status and progression of disease, and developed psychological correction techniques for myopes. However, until now, there have been no data on the efficacy of the techniques developed for psychological correction of maladaptive impairments in the late period after treatment. Purpose: To assess the long-term results of psychological correction of maladaptive individual psychological features in patients with myopia. Materials and Methods: Seventy one myopic and 43 emmetropic students were placed under observation. We used the following tools to determine individual psychological features: the Spielberger State Anxiety Scale adapted by Khanin, the Differential Personality Questionnaire adapted by the Bekhterev Institute, the Ellis Irrational Beliefs System, the Amirkhan’s Coping Strategy Indicator, the Bekhterev Institute Personality Questionnaire and the Structured Clinical Diagnostic Interview. Assessment of psychoemotional status was performed under rest conditions and under academic examination stress conditions. Myopic students were divided into three groups based on the results of psychodiagnostic testing. Cognitive behavioral, rational emotive, art and pharmacological therapies were used to treat them. A year after completion of this treatment, they received psychodiagnostic re-testing and repeated therapy. Results: Following the use of complex medical and psychological corrective treatment, the amount of psychological impairments in myopic students was found to be statistically significantly reduced, whereas the rate of the use of active coping strategies aimed at an individual’s independent problem solving was found to be increased. This improvement maintained during one year of observation, with an increase in the number of patients with a realistic response to disease. However, one year after this treatment course, the numbers of patients with high situational anxiety, as well as with asthenic and affective manifestations of a psychopathological syndrome increased, requiring repeated psychological corrective therapy. Conclusions: The use of the proposed algorithm for psychological support of myopic patients enables effective correction of their psychoemotional status. The procedure is performed in stages, with stages 1 to 3 involving (a) psychoemotional status testing, (b) determination of targets of and formation of groups for psychological corrective therapy, and (c) differential use of cognitive behavioral and rational emotive therapies, respectively. The efficacy and duration of therapeutic effect of treatment performed were found to be improved with timely use of repeated psychotherapeutic courses. Key words: myopia, individual psychological features, psychological correction Introduction A number of authors have reported on the impact of psychoemotional status on refractive development (and on development of myopia, in particular) in children [1]. The majority of healthy children aged 15-16 years with normal accommodative reserve have the weak type of nervous system (determined by the right-hand movement speed test) [2]. Compared to adolescents with slowly progressive myopia, those with rapidly progressive myopia were found to tend to descending (or weak) and intermediate types of dynamics of maximum arm movement tempo. The tendency identified above may evidence decreased lability of the nervous system (and, consequently, poor resistance to stress factors) in patients with rapidly progressive myopia [3]. Assessment of psychophysiological status based on the test of oculodynamic parameters of visual function enables the identification of individual features of brain neurodynamics, particularly through the analysis of individual’s visuospatial information as well as assessment of (a) different brain activity strategies, (b) personality, (c) emotional response pattern and (d) pattern of motor and sensory features [4]. Increased rates of myopia among schoolchildren and students drive the need for investigation of psychoemotional status and personality features in patients of this category. Progression of myopia in a pediatric or adolescent patient is asymmetric, with periods of rapid increase in axial (anteroposterior) length (and, consequently, in refraction) coinciding with periods of significant increase in anthropometric measurements. Previously, we have revealed that there may be a relationship between the myopic patient’s psychoemotional status and individual myopia progression rate, and developed the psychological correction techniques for myopes [5,6]. However, until now, there have been no data on the efficacy of the techniques developed for psychological correction of maladaptive impairments in the late period after treatment. The study purpose was to assess the long-term results of psychological correction of maladaptive individual psychological features in patients with myopia. Materials and Methods Seventy one myopic students (142 eyes) of the Odessa National Medical University (age, 17 years to 23 years; myopia, -1.0 to -10.0 diopters) were placed under observation. The control group comprised 43 emmetropic students (86 eyes). All these underwent routine ophthalmological examination. Conservative treatment was performed at University Clinic No. 2 of the Odessa National Medical University and included induction of phosphenes through electric stimulation of the retina, transpalpebral electrophoresis for delivery of spasmolytic agents, as well as neck and shoulder massage. The psychoemotional status was diagnosed and correction of maladaptive psychological features was performed at the Department of Psychiatry, Addiction, Psychological and Social Assistance, Odessa National Medical University. The period of clinical observation included sequential stages. At Stage 1 (Diagnosis Stage), after obtaining the informed concern, the student’s psychoemotional status was determined under academic examination stress. Situational anxiety was measured using the Spielberger State Anxiety Scale adapted by Khanin [7]. Individual’s personality features were assessed using the Differential Personality Questionnaire scale scores [8]. The Ellis test [9] and the Coping Strategy Indicator [10] were used to assess individual irrational attitudes and coping behavior, respectively. Patient's psychic response to somatic disease and maladaptive responses were assessed using the Bekhterev Institute Personality Questionnaire [11] and the Structured Clinical Diagnostic Interview [12, 13, 14, 15], respectively. At Stage 2 of clinical observation, based on the results of diagnostic assessments, psychological corrective therapy groups were formed. Cognitive behavioral, rational emotive, art and pharmacological therapies were used for psychological correction (Table 1). Group correction sessions were held weekly during four months in each observation group. In addition, students with marked psychoemotional impairments were prescribed 50-minute individual correction sessions twice weekly for a month; these sessions involved cognitive behavioral therapy and some elements of art therapy. In a number of cases, there was a need for incorporation of pharmacotherapeutics (mebicar perorally as per manufacturer’s instructions) into psychological correction regimen one month prior to and during academic examination period.
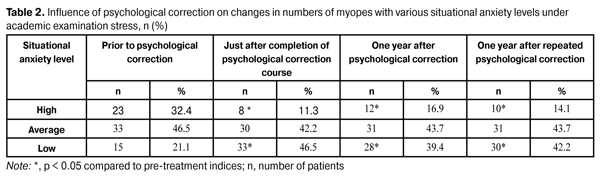
At Stage 3, after a five-month course of therapy, study subjects underwent psychodiagnostic re-testing during the next academic examination period. The results of studies conducted during Stages 1 to 3 have been reported previously [5, 6]. At Stage 4 of clinical observation, one year after completion of Stage 3, students underwent psychoemotional status re-testing using the tools mentioned above. They underwent a repeat course of psychological corrective therapy (if required) based on re-testing results. At Stage 5 of clinical supervision, one year after completion of Stage 4, myopic patients’ psychoemotional status was reassessed. Statistical analysis of the results was performed with the non-parametric tests [16]. Results and Discussion Previously, we have found that (1) psychoemotional features of myopic patients include high situational anxiety, prevalence of irrational attitudes, and low or average self-concept [5], and (2) these patients mostly have an anxious response to disease, tend to maladaptive manifestations of a psychopathologic syndrome, and generally assume non-active coping strategies [6]. Based on these findings, we designed the stages of psychocorrective support of myopic patients, and made an assessment of its efficacy [6]. A year after psychological corrective measures were taken, the number of patients with high situational anxiety under academic examination stress was found to be increased by 50.0% (Table 2). However, this number was statistically significantly reduced from the pre-therapy time point (р <0.05). All myopic patients under observation underwent a repeated course of psychological corrective measures and psychoemotional status re-testing one more year later. With this done, the number of patients with high situational anxiety under academic examination stress was found to be decreased, and was not statistically significantly different from that after the first psychological correction course. These findings suggest that systematic monitoring of myopic patients’ psychoemotional status and timely prescription of a repeated course of psychological corrective measures are essential for the long-term efficacy of psychological corrective therapy.
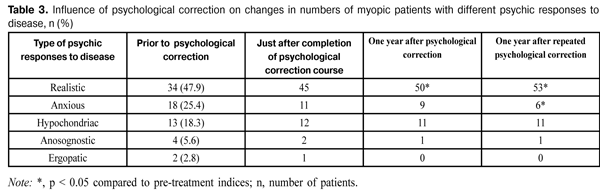
We found situational anxiety scores and patient's psychic response to disease to be interrelated. Thus, after psychological corrective measures were taken, a reduction in the number of patients with an anxious response to disease as well as an increase in that with a realistic response to disease (with patients understanding the condition and demonstrating a responsible attitude to treatment) was observed. One year after completion of the first psychological corrective course, no increase in the number of patients with an anxious response to disease was observed (Table 3). Patient's beliefs that the course of disease is unfavorable (with further progression of myopia), and that the treatment administered is ineffective and cannot stop progression of disease, along with anxiety about possible complications and serious non-compliance with medical treatment are characteristic of this response to disease.
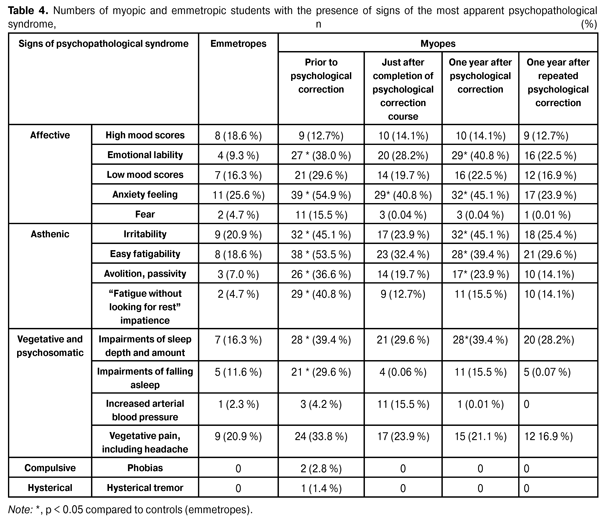
Additionally, we observed a decline in the numbers of patients with hypochondriac, anosognostic, or ergopatic response. The former patients give their minds too much to subjective and other unpleasant sensations (e.g., sensation of decreased visual acuity, especially under high visual load) and are always eager to talk to others about disease symptoms (often seek medical attention for visual acuity re-testing). Patients with anosognostic response to disease reject any thoughts about it and its effects, display a flippant attitude, ignore medical advice, and reject subjecting themselves to regular monitoring of myopia progression. Patients with ergopatic response to disease take a responsible attitude towards their disease and treatment, as well as towards monitoring of disease progression, due to their desire to preserve quality of life. It is possible that a statistically significant decrease in the number of patients with an anxious response to disease, as well as a decline in the numbers of patients with hypochondriac, anosognostic, or ergopatic response is associated with the use of active coping strategies by patients, resulting in reconsideration of the disease by the patient and in an increased belief in favorable outcome. The changes in prevailing coping strategies used by patients of three groups after completion of a series of corrective intervention sessions were also found to be stable. The number of patients using active coping strategies aimed at an individual’s independent problem solving did not change during one year of observation. After one year of observation, the patients were also assessed for signs of a psychopathologic syndrome. It is noteworthy that no compulsive or hysterical signs manifesting a psychopathologic syndrome were found. However, one year after completion of psychological corrective treatment, an increase in the numbers of patients with emotional lability, irritability, fatigue, as well as impaired sleep depth and amount was observed. These abnormalities were removed after taking a repeated course of psychological corrective measures (Table 4).
Conclusions The use of the proposed algorithm for psychological support of myopic patients enables effective correction of their psychoemotional status. The procedure is performed in stages, with Stage 1 involving diagnosis of patient’s psychoemotional status (assessment of self-concept, anxiety level, psychic response to disease, presence of irrational attitudes, coping strategies and symptoms of severity of a psychopathologic syndrome), Stage 2 involving determination of targets of and formation of groups for psychological corrective therapy, and Stage 3 involving differential use of cognitive behavioral and rational emotive therapies. The efficacy and duration of therapeutic effect of treatment performed were found to be improved with timely use of repeated psychotherapeutic courses as per indications. References
|