J.ophthalmol.(Ukraine).2019;6:29-33.
|
http://doi.org/10.31288/oftalmolzh201962933 Received: 25 October 2019; Published on-line: 06 January 2020 Efficacy of a novel non-contact corneal esthesiometer in assessing the neurotrophic status of the cornea in T1DM patients with bacterial keratitis O.V. Zavoloka,1 Cand Sc (Med); P.A. Bezditko,1 Dr Sc (Med), Prof.; O.O. Lukhanin,2 Cand Sc (Tech) 1 Kharkiv National Medical University; Kharkiv (Ukraine) 2 National Science Center “Kharkiv Institute for Physics and Technology”; Kharkiv (Ukraine) E-mail: Olesya_zavoloka@yahoo.com TO CITE THIS ARTICLE: Zavoloka OV, Bezditko PA, Lukhanin OO. Efficacy of a novel non-contact corneal esthesiometer in assessing the neurotrophic status of the cornea in T1DM patients with bacterial keratitis. J.ophthalmol.(Ukraine).2019;6:29-33. http://doi.org/10.31288/oftalmolzh201962933
Purpose: To develop a novel non-contact corneal esthesiometer and to determine the efficacy of this meter in assessing the neurotrophic status of the cornea in type I diabetic mellitus (T1DM) patients with bacterial keratitis. Material and Methods: We developed a novel non-contact corneal esthesiometer and determined the efficacy of this meter in assessing the neurotrophic status of the cornea based on examination of 30 T1DM patients with bacterial keratitis and 30 healthy individuals. Results: A corneal sensitivity assessment technique using our novel non-contact corneal esthesiometer was found to be non-invasive, accurate and repeatable. The use of low-temperature air jets in non-contact esthesiometry results in improved accuracy. Corneal sensitivity examination at nine specified points and calculation of mean corneal sensitivity threshold allows for a more comprehensive corneal function assessment, with account of the peripheral cornea. Conclusion: A significantly decreased corneal sensitivity was found in T1DM patients with bacterial keratitis. Our newly developed non-contact corneal esthesiometer was found to be effective in assessing the neurotrophic status of the cornea in T1DM patients with bacterial keratitis. Keywords: algesimeter, non-contact corneal esthesiometer, diabetes mellitus, bacterial keratitis
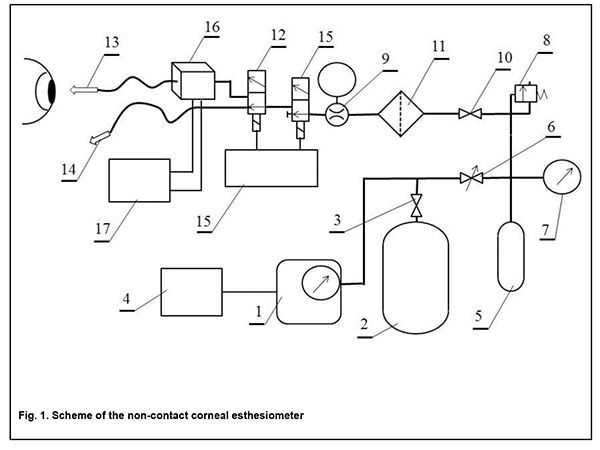
Introduction Bacterial keratitis is more common and runs a more severe course in patients with diabetes mellitus (DM) than in general population [1]. This may be due to neurotrophic corneas caused by the development of diabetic corneal neuropathy (a local manifestation of diabetic polyneuropathy) in patients with DM [2]. Efforts to measure corneal sensation date back to 1894, when von Frey used horse hair to test corneal sensation [3]. Nowadays, a special meter, algesimeter (or esthesiometer), is commonly used to provide more accurate and objective measurements of corneal sensation. Currently, the most popular and extensively used in the world algesimeter is the Cochet-Bonnet contact esthesiometer. The meter is based on the use of various lengths of a nylon filament to exert increasing amounts of pressure on the corneal surface. The nylon filament of 0.12 mm diameter is applied with an applicator onto the corneal surface to stimulate mechanonociceptors [4]. The Radzikhovskii contact algesimeter is the most commonly used in Ukraine, and its principle is as follows: three types of algesimeter (with masses of 2 mg, 10 mg and 50 mg, respectively) are in series put on the corneal surface for one second, and the examiner determines the mean number of corneal sensation points among nine specified points [5]. Contact esthesiometers, however, have a number of substantial disadvantages such as the contact nature; restrictive stimulation of only mechanoreceptors, user-dependency; limited stimulus intensity range; variation in stimulus delivered; lack of reproducibly measuring corneal sensation at low thresholds of stimuli; effect of a physiological blink reflex induced as the meter approaches the eye; and difficulties with sterilization [6]. Because of the disadvantages of the Cochet-Bonnet esthesiometer, efforts were made to develop noncontact and more accurate corneal esthesiometers. The Belmonte esthesiometer is among the newer devices that are built upon the principle of the noncontact pneumatic esthesiometry; a jet of air stimulates corneal nerves by compressing the surface [7]. Unlike the Cochet-Bonnet esthesiometer, its modified version, the CRCERT-Belmonte esthesiometer, allows corneal sensation to be quantitatively assessed at air jet temperatures ranging from 20 to 34 °C, with stimulation of not only mechanoreceptors (A? type), but also cold receptors (A? and C type) that are activated with the corneal surface temperature reduced below 33 °C. A limitation of this meter is its low efficacy due to a limited range of air jet temperatures (20-34 °С), which reduces its value in assessing the function of corneal cold receptors. Another limitation is that only corneal sensitivity in the central cornea, but not in the peripheral cornea can be assessed, and thus the corneal sensitivity cannot be averaged over the entire cornea. In addition, to date, there is not any noncontact esthesiometer available in Ukraine. Therefore, there is a need for the development of an advanced noncontact esthesiometer for more accurate measurements of corneal sensitivity which is important for assessing the neurotrophic cornea in patients with DM and bacterial keratitis. The purpose of the study was to develop a novel non-contact corneal esthesiometer and to determine the efficacy of this meter in assessing the neurotrophic status of the cornea in type I diabetic patients with bacterial keratitis. Material and Methods We developed a non-contact corneal esthesiometer (Fig. 1), which is composed of a compressor (1) for pressurizing the air flow, and receiver (2) for accumulating the pressurized air in amount required for more than one-hour continuous operation. The compressor is equipped with a pressure gauge and safety pressure relief valve set at a pressure of 6 atmospheres (atm). The receiver can be turned off with a valve (3) for the long-term storage of air or other gases. The compressor is powered from a power unit (4). The air flow is stabilized by making a constant pressure of 0.05 atm in a surge tank (5) with the help of a reducer (6). A pressure gauge (7) monitors the pressure, and a safety pressure relief valve (8) is activated should the pressure in the surge tank exceed 0.1. The air flow ranging from 18 cm3/min to 240 cm3/min (0.3 cm3/second to 4 cm3/second) is measured by a flow meter (9) and regulated by a control valve (10). Air is additionally cleared from dust and sprays in a filter (11). A three-way solenoid valve (12) is used to form one to eight air jet impulses lasting for 0.5-2 sec, with a 0.5-2 sec inter-impulse interval, and to direct the air flow to a primary nozzle (13) or a similar secondary nozzle (14). The air flow switching method and the solenoid with a short switching time provide for (a) reduction in transients associated with changes in pressure in the air flow and (b) similarity and uniformity in velocity among all air jet pulses. Air jet impulse duration and inter-impulse interval for the primary nozzle can be set up in increments of 0.5 sec with accuracy of 10%. In order to remove the first transient process before supplying air to the operating nozzle, an auxiliary solenoid valve (15) is made open 3 seconds before opening the primary solenoid valve. The auxiliary solenoid valve helps reducing air losses, thus increasing the duration of equipment operation without supplying additional air to the receiver. A pulse generator (15) is provided to control operation of solenoid valves by producing a pre-set number of pulses of pre-set duration and pulse-to-pulse period to be applied to the primary solenoid valve. The leading edge of the pulse applied to the auxiliary solenoid valve advances the leading edge of pulse applied to the primary solenoid valve by 3 seconds, whereas the trailing edge of the former pulse coincides in time with the trailing edge of the latter pulse. In addition, pulse generation can be stopped at any time, and air can be supplied continuously to the operating nozzle to determine and re-set the air flow. An air conditioner (16) with temperature controller (17) is used for setting the air temperature in the range 5–40оС. The device has the following characteristics: air flow velocity along the air jet axis, 0–4 m/s; air velocity measurement error, ± 20%; air jet impulse duration, 0.5 sec, 1 sec, 1.5 sec, and 2 sec; inter-impulse interval, 0.5 sec, 1 sec, 1.5 sec, and 2 sec; number of jet impulses, 1, 2, 3, 4, 5, 6, 7, 8; air flow, 0.3–4 cm?/s; air jet temperature (with operating air conditioner), 5-40°С; nozzle diameters, 0.5, 1.0, 1.2, 1.5 mm; power supply voltage, 220±10% V; power consumption, ?200 W; minimum pressure in the receiver, 6 atm; duration of continuous operation, ? 1 hour.
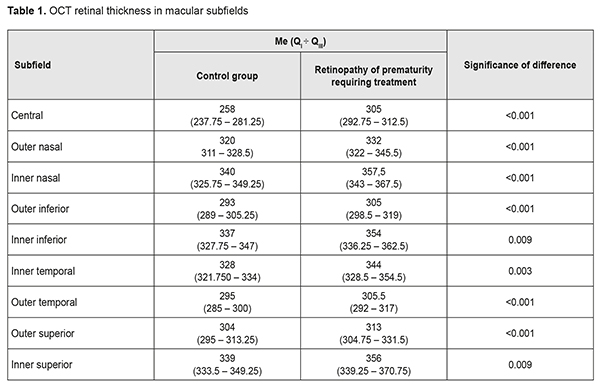
The set-up procedure of using the novel non-contact corneal esthesiometer is as follows. Before examining corneal sensation, apply power voltage (220 V) to compressor power unit (4), pulse generator (15), and, if required, to air conditioner controller (17). Use the compressor (2) to make a pressure of 6 atm in the receiver (2). Make a pressure of 0.05 atm in the surge tank (5) with the help of the reducer (6). Turn on the pulse generator (15), activate the air-flow setting mode, and set the required air flow rate. Stop the air flow. Set the required number of air jet impulses, air jet impulse duration, and inter-impulse interval. Place the primary nozzle at the required distance from one of the corneal sensation examination points. Thirty healthy volunteers (16 women and 14 men) aged between 18 and 50 years and 30 T1DM patients with bacterial keratitis (13 women and 17 men) aged between 18 and 49 years were enrolled in the study to determine the efficacy of the novel non-contact corneal esthesiometer. The study protocol was approved by the bioethics committee of Kharkiv National Medical University (protocol No.11 issued on December 5, 2018). Corneal sensation was assessed at nine specified examination points (superior, superior nasal, superior temporal, nasal, central, temporal, inferior nasal, inferior temporal, and inferior points), and average corneal sensitivity threshold was determined. The following parameters for the novel non-contact air-jet corneal esthesiometer were used: diameter of air jet output orifice, 0.5 mm; pulse duration, 1 s; distance to the corneal surface, 4 mm; and air jet temperature, 5, 15, 20, 30, 40 °С. The minimum air jet force was used initially. Thereafter, the air jet force was gradually increased until the subject reported a sensation of breeze. Each experiment was performed ten times to assess the reproducibility of the technique. Subsequent experiments at the same corneal sensation examination point were separated by a time interval of at least one minute to avoid the effect of adaptation or summation. Subsequent corneal sensation experiments at different air jet temperatures were separated by a time interval of at least 20 minutes to provide for an adequate balance of receptors before changing the temperature of the stimulus. Parametric and non-parametric statistical methods were used for statistical analyses. The coefficient of repeatability, r, was defined as ±1.96 ?d where ?d represents the sample standard deviation of the differences between the paired measures. Results and Discussion In healthy individuals, average corneal sensitivity threshold, as assessed by non-contact esthesiometry with air jet of 5°С, varied from 28.3 to 62.6 mL/min (mean value, 47.3 ± 8.9 mL/min; coefficient of repeatability, 15.3) (Table 1), and, as assessed with air jet of 15°С, varied from 34.3 to 74.5 mL/min (mean value, 52.9 ± 9.1 mL/min; coefficient of repeatability, 17.5). In addition, in healthy individuals, average corneal sensitivity threshold, as assessed with air jet of 20 °С, varied from 38.2 to 76.2 mL/min (mean value, 57 ± 9 mL/min; coefficient of repeatability, 19.1) (Table 1), and, as assessed with air jet of 30°С, varied from 50.2 to 98.6 mL/min (mean value, 72 ± 9.8 mL/min; coefficient of repeatability, 26.2). Moreover, in healthy individuals, average corneal sensitivity threshold, as assessed with air jet of 40 °С, varied from 57.9 to 101.4 mL/min (mean value, 78.3 ± 9.1 mL/min; coefficient of repeatability, 28.1).
In T1DM patients with bacterial keratitis, average corneal sensitivity threshold, as assessed by non-contact esthesiometry with air jet of 5°С, varied from 101.4 to 154.7 mL/min (mean value, 127.9 ± 15.7 mL/min; coefficient of repeatability, 14.1) (Table 1), and, as assessed with air jet of 15°С, varied from 111.5 to 159.6 mL/min (mean value, 135.2 ± 14.5 mL/min; coefficient of repeatability, 15.2). In addition, in T1DM patients with bacterial keratitis, average corneal sensitivity threshold, as assessed with air jet of 20 °С, varied from 119.8 to 167.8 mL/min (mean value, 143.8 ± 14.9 mL/min; coefficient of repeatability, 16.9) (Table 1), and, as assessed with air jet of 30°С, varied from 127.3 to 174.8 mL/min (mean value, 152.4 ± 14.2 mL/min; coefficient of repeatability, 18.3). Moreover, in T1DM patients with bacterial keratitis, average corneal sensitivity threshold, as assessed with air jet of 40 °С, varied from 135.8 to 182.4 mL/min (mean value, 159.5 ± 14.2 mL/min; coefficient of repeatability, 19.6). Both in T1DM patients with bacterial keratitis and in healthy individuals, at any air jet temperature, the lowest corneal sensitivity threshold was found in the central corneal point, and the highest sensitivity threshold was found in the inferior corneal point (p < 0.05). At any air jet temperature, mean corneal sensitivity threshold in T1DM patients with bacterial keratitis was significantly higher than in healthy individuals. Thus, at air jet temperature of 5°С, 15 °С, 20 °С, 30 °С, and 40 °С , mean corneal sensitivity threshold in T1DM patients with bacterial keratitis was 2.7-fold, 2.6-fold, 2.5-fold, 2.1-fold, and two-fold, respectively, higher than in healthy volunteers (р < 0.05). Therefore, a corneal sensitivity assessment technique using our novel non-contact air-jet corneal esthesiometer was found to be non-invasive, accurate and repeatable. The use of low-temperature air jets in non-contact esthesiometry results in improved accuracy, since it provides for effecting not only mechanonociceptors, but also cold receptors (i.e., nerve filaments of two types, type A? and C). Corneal sensitivity examination at nine specified points and calculation of mean corneal sensitivity threshold allows for a more comprehensive corneal function assessment, with account of the peripheral cornea. A significantly decreased corneal sensitivity was found in T1DM patients with bacterial keratitis, which could result from mixed impairment of the neurotrophic status of the cornea due to bacterial inflammation developing in the presence of diabetic corneal neuropathy. Conclusion
A corneal sensitivity examination technique using our novel non-contact corneal esthesiometer was found to be non-invasive, accurate and repeatable, and can be used for assessing the neurotrophic status of the cornea in T1DM patients with bacterial keratitis.
References 1.Vieira-Potter VJ, Karamichos D, Lee DJ. Ocular complications of diabetes and therapeutic approaches. Biomed Res Int. 2016;2016:3801570. 2.Bikbova G, Oshitari T, Baba T, Yamamoto S. Neuronal Changes in the Diabetic Cornea: Perspectives for Neuroprotection. Biomed Res Int. 2016;2016:5140823. 3.Von Frey M. Berichte uber die verhaindlungen der koniglich sachsichen. Ges Wiss. 1894;46:185–96. 4.Cochet P, Bonnet R. L’esthesie corneenne. La Clin Ophtalmol. 1960;4:3–27. 5.Radzikhovski? BL, Luchik VI. [Corneal sensitivity and its diagnostic value in ocular and systemic disease]. Kyiv: Zdorov’ia; 1974. Russian. 6.Golebiowski B, Papas E, Stapleton F. Assessing the sensory function of the ocular surface: implications of use of a non-contact air jet aesthesiometer versus the Cochet-Bonnet aesthesiometer. Exp Eye Res. 2011; 92:408–13. [PubMed: 21376718] 7.Murphy PJ, Patel S, Marshall J. A new non-contact corneal aesthesiometer (NCCA). Ophthal Physiol Opt. 1996;16:101–7.
The authors certify that they have no conflicts of interest in the subject matter or materials discussed in this manuscript.
|