J.ophthalmol.(Ukraine).2015;5:30-34.
|
https://doi.org/10.31288/oftalmolzh201553034 The level of interferons ? and ? in the blood of patients with uveitis of different clinical characteristic and course of the disease N.V. Konovalova Chaibi Abderrahim Filatov Institute of Eye Diseases and Tissue Therapy, Odessa, (Ukraine) Introduction. Social importance of uveitis is determined by high frequency of occurrence, affection of persons mainly of work ability age, high frequency of disability due to vision. Objective. To determine the peculiarity of interferons ? and ? expressions in the blood of patients with uveitis of different clinical characteristic and course of the pathological process. Materials and methods. There were examined 61 patients with uveitis of different localization (anterior and posterior), clinical course (chronic and acute), degree of severity (severe and moderate) and differential diagnosis (iridocyclitis, focal and disseminated chorioretinitis, neuritis, panuveitis) who were examined ophthalmoscopically (ophthalmoscopy, tonometry, visometry). 59 people were determined the level of interferons ? and ? in the blood plasma by the method of the immune enzyme analysis. Results. There was determined peculiarity of interferons ? and ? expressions in the blood of patients with uveitis of different clinical characteristic and course peculiarities of the pathological process. It is shown that the content of these cytokines are significantly lower in posterior uveitis as well as in the chronic course with high degree of reliability. There was found a reliable correlation between the level of interferons under the study and above mentioned characteristics. The degree of uveitis severity does not correlate with the level of interferons in the patients’ blood as well as there was no revealed association between the average values of concentration of interferons ? and ? in the blood of the patients with uveitis taking into account the differential diagnosis. Conclusions. The data obtained prove the role of interferons ? and ? in development of uveitis and may be of interest for determining the character of the course of the pathological process and treatment efficacy. Key words: uveitis, clinical characteristic, course, interferons ? and ?, blood plasma
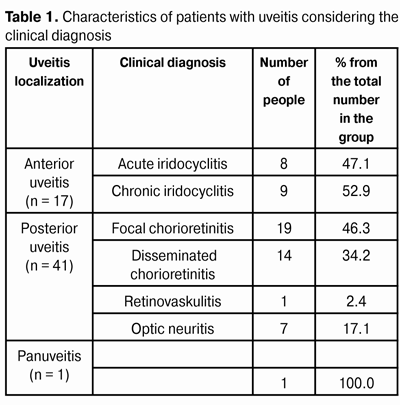
Introduction High social significance of endogenous uveitis problem is determined by a significant frequency of the disease occurrence, primary affection of young and working age people, temporary disability due to long-term disease progress and its relapses, as well as frequent disablement due to vision problems [16]. Uveitides constitute 7-30% of general structure of eye diseases and cause blindness in 5-18% of cases [10,11]. Immunopathology is one of the key etiopathogenic factors of inflammatory diseases of the retina and choroid. Frequent causes of endogenous uveitis are chronic or acute infections characterized by shifts in almost all sectors of natural and adaptive immunity: tuberculosis, toxoplasmosis, herpes simplex, cytomegalovirus, influenza, enteroviruses and hepatitis B virus [20]. Immune disorders can be both a prerequisite and a consequence of an infectious process. Uveitis is characterized by stimulation of local and/or systemic production and violation of the pro- and anti-inflammatory cytokines balance, defects in the system of interferons (IFN): deficit or, on the contrary, over-production of IFN-? and/or IFN-?, T-cell immunity weakening, especially its helper unit, circulating immune complexes increase, etc. Cytokines are the regulatory peptides carrying out the formation and regulation of host defense reactions participating in the immune response and providing intercellular interactions. The biological effect of cytokines is versatile under the influence of various pathogenic factors [6]. An important role in the development of innate and adaptive immunity against different infectious agents is for the proinflammatory cytokines, which in contact of immunocompetent cells with factors causing an inflammation are activating the granulocytes, macrophages, endothelial cells [19]. An important role in ulcerative antiviral immune response is for interferons (IFN). The main directions of the biological action of IFN-? are antiviral and tumorocidal actions, resulting in an inhibited tumor growth, reproduction of viruses in cells, increased antiviral, antimicrobial, anti-parasitic resistance, as well as stimulated antiviral activity of IFN-? [17]. Producers of IFN-? are activated TH-1 lymphocytes and natural killer cells. The inducers of its synthesis are viruses, bacteria, toxins, metabolites, some vegetable proteins and mitogens [18]. Increased IFN-? concentration level may be observed in acute viral, bacterial and parasitic infections, in exacerbation of diseases of the gastrointestinal tract [18], in the blood of patients with bronchial asthma and multiple sclerosis [2, 20]. Upon activation of viral infection during pregnancy the level of IFN-? in amniotic fluid in contrast is decreased 2.5 times compared with health objects [14]. IFN-? amplifies the antiviral resistance, inducing the enzymes synthesis, that suppress the formation of nucleic acids and proteins of viruses, has the immunomodulating effect and increases the expression of a major histocompatibility complex in cells [1,20]. IFN-? is synthesized mainly by leukocytes (B-lymphocytes, monocytes), although it may be produced by any type of cell in response to the agitation [18]. Its inducers include viruses and their products, bacteria, mycoplasma and protozoa, other cytokines and growth factors (IL-1, IL-2, TNF-?, colony-stimulating factors) [22]. IFN-? content changes in patients with hepatitis and liver cirrhosis of viral etiology [7,13,15]. During exacerbation of viral infections its concentration increases significantly, and decreases during the convalescence period. The dependence between the level of IFN-? in blood and the severity and duration of influenza is showed [3]. Systemic IFN-? concentration increase occurs in autoimmune diseases [21], aggravation of peptic ulcer and cholelithiasis [18]. Proinflammatory cytokines analysis can result in useful information for the diagnosis, dynamics monitoring and treatment of infectious and inflammatory diseases. Objective is to determine the peculiarity of interferons ? and ? expressions in the blood of patients with uveitis of different clinical characteristic. Material and methods There were examined 61 patients of 13-76 age with uveitis diagnosis in the Department of Eye Inflammatory Pathology of State Institution "The Filatov Institute of Eye Diseases and Tissue Therapy of the National Academy of Medical Sciences of Ukraine''. The average age was (38.1 ± 13.2) with 33 (54.1%) women and 28 (45.9%) men among them. In the instruction of CJSC "Vector-Best" (Novosibirsk, Russia) on the determination of IFN-? content in blood the normal correlation range is 0-5 pg/ml. The results of extensive studies with the use of cytokines line reference values determination kits have shown that the content of IFN-? in blood ranged within 0-86 pg/ml total among the group (152 donors). 80.3 % examined patients had the corresponding values within 0-5 pg/ml, with average value of (4.8 ± 0.96) pg/ml. And 19.7% had increased values of (> 5 pg/ml) [6]. As for IFN-?, the range of concentrations of this cytokine in the blood was 0-84 pg / ml, while normal concentration is 0-25 pg / ml with the average value of 9 pg / ml [17]. Clinical characteristics of patients with interferons level determined are shown in Table 1.
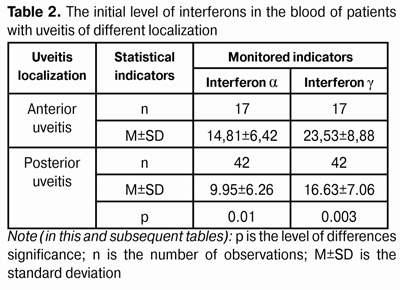
Distribution of the patients considering the etiological factors was presented in details previously [12]. Patients’ examination was made with the use of standard ophthalmological research protocol, which includes ophthalmoscopy, tonometry, visometry. Determination of interferons ? and ? level was made in blood plasma for 59 patients with enzyme linked immunosorbent assay using reagents set for the quantitative evaluation of interferons ? and ? in human biological fluids (Vector-Best, Novosibirsk, Russia) and registration of the results through the spectrophotometry at a wavelength of 450 nm [8, 9]. The obtained data was statistically processed with the use of Statistica 7.0 software and the parametric Student criterion for pair wise comparison of two groups and preliminary assessment of distribution normality, Kruskal-Wallis criterion in case of simultaneous comparison of more than two groups, as well as Spearman rank correlation criterion [4]. Results and discussion The initial level of examined IFN-?, and -? in blood of patients with uveitis in whole for the group (n = 59) was (11.19 ± 6.60) pg / ml and (18.39 ± 8.07) pg / ml, respectively, that exceeds the level of IFN in the blood of healthy individuals (according to the literature). The next phase of research was to determine the characteristics of IFN expression in patients with uveitis, depending on the clinical characteristics of the disease. Determination of IFN-? and - ? level in blood of patients with uveitis considering the localization of inflammation (Table 2) showed that the content of these cytokines was significantly lower under the pathological process in the posterior eye section 1.5 and 1.4 times for IFN-? and-?, respectively (p < 0.05 in both cases).
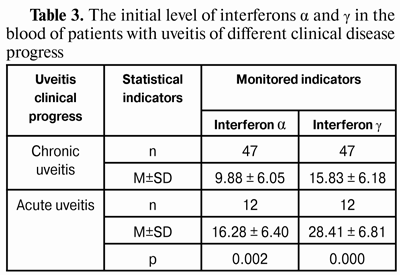
Note (in this and subsequent tables): p is the level of differences significance; n is the number of observations; M±SD is the standard deviation Analysis of the data on the source level of the investigated IFN flow, depending on the nature of the pathological process (Table 3) revealed pronounced reduction of these indicators in chronic uveitis regarding such data when sharp course of the disease, 1.7 and 1.8 times, respectively (significance level differences p < 0.002).
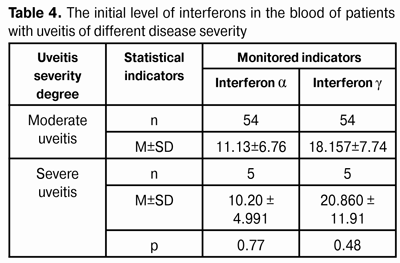
An attempt to evaluate uveitis severity on the basis of IFN level data in patients' blood has not revealed any connection between these parameters (Table 4). Interferon ? content was insignificantly lower (9.1%), and interferon ? - by 14.9% higher among persons with severe uveitis compared to the corresponding data at an average severity of the disease. However, the heterogeneity of the studied groups on quantitative composition should be noted. There were significantly less patients with severe uveitis (by 11 times), than patients with moderate disease (5 and 54 persons, respectively), that may be an explanation of the lack of differences expression between these groups.
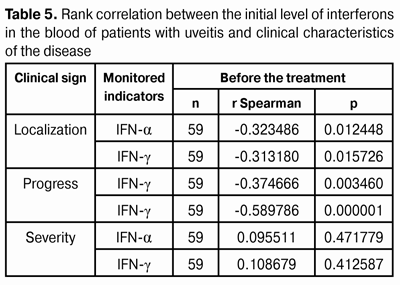
An attempt to correlate the expression level of clinical signs of the disease with the content of interferons ? and ? in the blood of patients with uveitis has revealed the presence of reliable correlative connection according to nonparametric Spearman rank criterion between examined IFN and the localization of the pathological process and the nature of its progress and severity (Table 5).
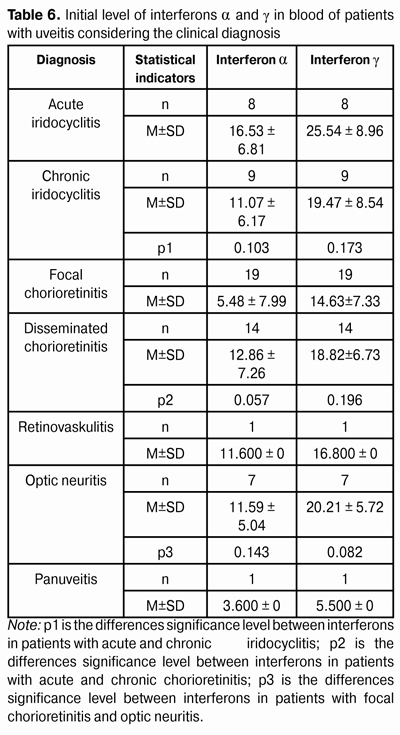
During the analysis of the average values of interferons content in the blood of patients with uveitis, considering the clinical diagnosis, it was found, that in all cases IFN-? content was lower than IFN-? content (Table 6). Pairwise comparison of relevant indicators in pairs in groups of patients with acute and chronic iridocyclitis, focal and disseminated chorioretinitis and focal chorioretinitis and optic neuritis, has revealed the presence of reliable correlative connection on non parametric Spearman rank criterion between the level of examined interferons and localization of the pathological process, the character of its progress and exacerbations presence. However, there was found an expressed tendency of IFN content increase during the treatment of acute process in the anterior eye segment. And the lowest value of relevant indicators was observed in a patient with panuveitis as the most serious manifestation of the inflammatory process. During the analysis of all data concerning the level of IFN-? and IFN-? in blood of patients with uveitis considering the clinical diagnosis (focal or disseminated chorioretinitis, optic neuritis, retinovaskulitis, panuveitis), with the use of Kruskal-Wallis criterion there was found no reliable correlation between the average values of these cytokines concentration (?2= 5.8402, df = 6, p = 0.441 in case of IFN ? and ?2= 9.230, df = 6, p = 0.161-IFN ?).
Conclusions 1. Interferons ? and ? content in the blood of patients with uveitis is more significantly decreased in the pathological process of the posterior eye section, than in anterior uveitis (1.5 and 1.4 times respectively at p < 0.05 in both cases). 2. There was found a substantial decrease of interferons ? and ? level in the blood of patients with chronic uveitis regarding such data in acute disease progress sharp course of the disease (1.7 and 1.8 times respectively at p < 0.002). 3. Uveitis severity does not correlate with the interferons level in the blood of patients: interferon ? content insignificantly (by 9.1%) lower, and interferon ? content - higher by 14.9% in patients with severe uveitis compared to corresponding data at an average severity of the disease. 4. Reliable correlation connection was found between the level of examined interferons and pathological process localization, the nature of its progress and severity. 5. No reliable correlation connection was found between the average concentrations of interferons ? and ? in the blood of patients with uveitis depending on clinical diagnosis (focal or disseminated chorioretinitis, optic neuritis, retinovaskulitis, panuveitis) by Kruskal-Wallis criterion (?2= 5.8402, df = 6, p = 0.441 for interferon ? and ?2= 9.230, df = 6, p = 0.161 for interferon ?). Literature 1.Vorobieva AA. [Medical microbiology, virology and Immunology atlas]. M.: MIA. 2003; 195. Russian. 2.Bakirov AB, Shagalina AU, Fukalova LA. In: Bakirov AB., Shagalina AU., Fukalova LA. Tsitoksiny i vospalenie. 2002; 2: 92. Russian. 3.Vasilyeva IA, Jchahov AV, Trofimov AV. In: Vasilieva IA, Jchahov AV, Trofimov AV. Tsitoksiny i vospalenie. 2003; 2: 51-57. Russian. 4.Glanz S. [Biomedical statistics]: translation from English. M.: Practice; 1998. 459. Russian. 5.Ershov FI. [Interferon system in normal and pathological condition]. M.: Meditsina; 1996. 72. Russian. 6.Zaitseva GA, Vershynina OA, Matrohina OI, Senkina EA, Karpova MV. [Cytokine status of blood donors and its components]. Fundamentalnye issledovaniya. 2011; 3: 61-65. Russian. 7.Zmyzgova AV. [Interferon therapy of viral hepatitis]. M: 1999; 234. Russian. 8.Instruction for using the kit of reagents for quantitative determination of human alpha interferon in biological fluids and human culture mediums. ZAO "Vector-Best'': Novosibirsk; 30.05.08. 22. Russian. 9.Instruction for using the kit of reagents for quantitative determination of human gamma interferon in biological fluids and human culture mediums. ZAO "Vector-Best'': Novosibirsk; 30.05.08. 22. Russian. 10.Katargina LA, Hvatova AV. [Endogenous uveitis in children and adolescents]. M.: Meditsina; 2000. 320. 11.Katsnelson LA., Tankovskyy VE. [Uveitis]. M.: 4 filial Voenizdata; 1998. 208. Russian. 12.Konovalova NV, Abderrahim Shaibi. [Cellular and humoral immunity in patients with uveitis]. Oftalmol. Zh. 2015; 2: 34-36. Russian. 13.Kuznetsov SI, Latash VG. Meditsinskaya immunologiya. 2002; 2: 364-365. Russian. 14.Makarov OV, Bachareva IV. Fundamentalnye issledovaniya. М.: Akademiya Yestestvoznania. 2004; 1: 67. 15.Mamaev SN. Klinicheskaya i laboratornaya diagnostika. 2001; 8: 45-47. Russian. 16.Neverova EA. Pathogenetic substantiation of ozone use in endogenous uveitis. In: Dissertation. of Candidate of Medical Sciences 14.00.16 Patologicheskaya fiziologiya. 2007; Saransk: 116. Russian. 17.Riabicheva TG, Varaskin NA, Timofeeva NV. Rukavishnikov MJ. Determination of cytokines with the use of enzyme immunoassay method ZAO Vector-Best. Inform. bulleten Novosti "Vector-Best”. 4 (34). December 2004 Available at: http://www.vector-best.ru/nvb/n34/st34_4.htm. Russian. 18.Tsaregorodtseva TM, Serova TI. Cytokines in Gastroenterology. M.: Anakharsis; 2003. 50. Russian. 19.Razavi NL. Proinflammatory cytokines in response to insulin-induced 20.hypoglycemic stress in healthy subjects. Metabolism. 2009; 58 (4): 443-448. 21.Fields Virology / ed. David M. Knipe. Philadelphia: «Lippincott Williams & Wilkins». 2001; 1: 321–353. 22.Grau G, Roux-Lombard P, Gyster C. Immunol. 1989; 68: 196–198. 23.The Cytokine Handbook. Ed. Thomson AW and Lotze MT. London, San Diego: Academic Press. 2003.
|