J.ophthalmol.(Ukraine).2017;6:3-6.
|
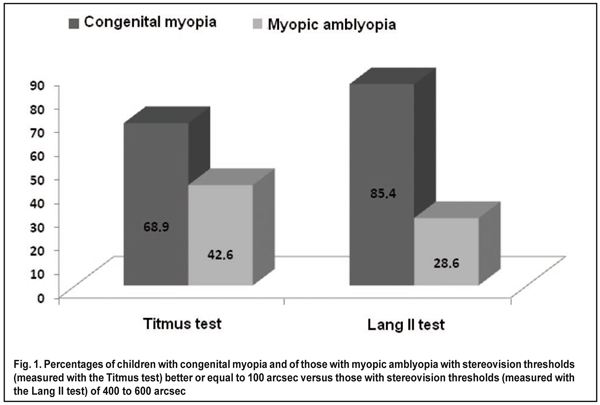
https://doi.org/10.31288/oftalmolzh2017636 Stereovision in children with congenital myopia and in those with myopic amblyopia A.Iu. Mukhina1, Post-grad Student, I.M. Boichuk2, Dr Sc (Med), L.D. Zhuravliova1, MD 1Regional Pediatric Clinical Hospital 2Filatov Institute of Eye Disease and Tissue Therapy Ivano-Frankivsk, Odessa, Ukraine E-mail: iryna.ods@gmail.com Background: Stereovision is a reliable and sensitive indicator of the ability to analyze spatial relationships. The ability to fuse images that fall on either corresponding or slightly disparate retinal elements within Panum’s fusional area results in binocular appreciation of visual object in depth (i.e. in the third dimension) and in the ability to orientate oneself in space. While studying the pathophysiological mechanisms of abnormal visual function, scientists analyze the system at the level of an individual channel, and investigate the interaction between channels. Despite the progress made so far in studying stereovision, it is not known whether the stereoacuity test scores for children with congenital myopia differ from those for children with myopic amblyopia in the absence of fundus changes. Purpose: To investigate stereovision in children with congenital myopia and in those with myopic amblyopia with the use of various stereoacuity tests. Materials and Methods: We studied 52 children (104 eyes; age, 5 to 18 years) who were under observation. These included children with amblyopia (54 eyes) and myopes without amblyopia (50 eyes). Mean myopia in children with amblyopia was somewhat higher than in those with congenital myopia (7.01 ± 4.2 D vs 6.5 ± 4.0 D). In total, 22 eyes had astigmatism greater than 4.0 D, and 7 eyes had anisometropia greater than 2.0 D. Mild amblyopia (with BCVA greater than 0.4), moderate amblyopia (with BCVA of 0.2 to 0.4) and severe amblyopia (with BCVA of 0.05 to 0.15) was found in 32 eyes, 9 eyes, and 9 eyes, respectively. Results: In 68.9% of children with congenital myopia, the stereo threshold measured with Titmus contour tests was ? 100 arcsec. In addition, in 85.4% of children with congenital myopia, the stereo threshold measured with Lang II random-dot test was 400 to 600 arcsec. The length of time till the occurrence of a stereo effect in 84.2% of children was less than 20 s. Conclusions: Stereovision was better in children with congenital myopia than in those with myopic amblyopia. Contour and random-dot stereotests found that the former children had better stereovision than the latter. A length of time (from presentation of a test object to the occurrence of a stereo effect) of less than 20 s was found in 88.46% of children with congenital myopia, and in 16.6% of those with myopic amblyopia. Keywords: congenital myopia, myopic amblyopia, stereo vision, Lang II random-dot test, Titmus stereo fly test, binocular functions Introduction Stereoscopic vision is a reliable and sensitive indicator of the ability to analyze spatial relationships. Belostotskii [1] believes that the ability of the visual system to appreciate correctly the third spatial dimension (i.e., depth perception) is essential for the complex process of binocular spatial perception. The ability to fuse images that fall on either corresponding or slightly disparate retinal elements within Panum’s fusional area results in binocular appreciation of visual object in depth and in the ability to orientate oneself in space [1, 2]. While studying the pathophysiological mechanisms of abnormal visual function, scientists analyze the system at the level of an individual channel, and investigate the interaction between channels [3, 4]. In myopia, the need for accommodation is diminished or eliminated, and therefore, the stimulus for convergence is reduced. In low potential for fusion, bifixation mechanism exerts no control over convergent and divergent movements, concomitant strabismus emerges, and the development of stereoscopic vision becomes abnormal [5]. Binocular vision abnormalities are one of the most important issues in pediatric ophthalmology, with their prevalence in children being about 1.5-2.5%. Visual acuity of at least 0.4 in the worst eye, no great difference in visual acuity between the right and left eyes, symmetrical arrangement of eyes, and no marked anisoaccommodation are the conditions required for the development of binocular vision [2]. Most clinical stereoacuity tests are based on the creation of lateral disparity through shifting left-hand and right-hand images of a test object while (a) presenting paired pictures in a lens stereoscope, or (b) demonstrating disparate images with the use of color, polarized or liquid crystal spectacles under conditions of separated vision fields of the left and right eyes. Other tests (e.g., those of the Litinskii eye depth measurement apparatus and three-rod devices of various designs [6, 7]) are based on the use of actual difference in depth, with tests objects varying in depth arrangement. Of special note are the following clinical stereoacuity tests: the Lang test, Titmus test, Pulfrich effect images, etc. [8, 9]. Computer-generated Julesz random-dot stereograms have been used since 1960 to study stereopsis. Studies are underway investigating stereopsis with random-dot stereograms of various spatial frequencies. This research has been substantiated by studies of DeAngelis, Ohzawa and Freeman which considered the mechanisms for the extraction of depth information by neurons in the striate cortex receiving binocular input and having simple or complex receptive fields [10]. As the first stage of processing of binocular information in the visual system is related only to the visual cortex, one could expect some difference in the perception of spatial-and-frequency characteristics of various stereoacuity tests between visual cortex disorders and disorders of other visual subsystems (e.g., the retina or optic nerve) [11]. Despite the progress made so far in studying stereovision, it is not known whether the stereoacuity test scores for children with congenital myopia differ from those for children with myopic amblyopia in the absence of fundus changes. Answering this question with allow us to diagnose these diseases more accurately. The purpose of this study was, therefore, to investigate stereovision in children with congenital myopia and in those with myopic amblyopia with the use of various stereoacuity tests. Materials and Methods We studied 52 children (104 eyes; age, 5 to 18 years) who were under observation. These included children with amblyopia (54 eyes) and myopes without amblyopia (50 eyes). Mean myopia in children with amblyopia was somewhat higher than in those with congenital myopia (7.01 ± 4.2 D vs 6.5 ± 4.0 D). In total, 22 eyes had astigmatism greater than 4.0 D, and seven children had anisometropia greater than 2.0 D. In addition, mild amblyopia (with BCVA greater than 0.4), moderate amblyopia (with BCVA of 0.2 to 0.4) and severe amblyopia (with BCVA of 0.05 to 0.15) was found in 32 eyes, 9 eyes, and 9 eyes, respectively. All patients had stereopsis. They underwent a routine clinical eye examination including visual acuity, biomicroscopy, refractometry, and ophthalmometry. In addition, they had the type of their binocular vision determined with the color test and synophophore. Stereoscopic vision was assessed with Lang-Stereotest II and Titmus Circle and Animal tests at daylight at a viewing distance of 30 cm, under conditions of best-corrected vision. The length of time from presentation of a test object to the reaction of the individual was determined with a stopwatch. STATISTICA 8 software was used for statistical analysis. Data without homogeneity of variance were analyzed with one-way ANOVA, and multiple post hoc comparisons were performed using the Newman–Keuls correction or chi2 test for contingency table analysis. Results In 68.9% of children with congenital myopia, the stereo threshold measured with Titmus contour tests was ? 100 arcsec. In addition, in 85.4% of children with congenital myopia, the stereo threshold measured with the Lang II random-dot test was 400 to 600 arcsec (Fig. 1).
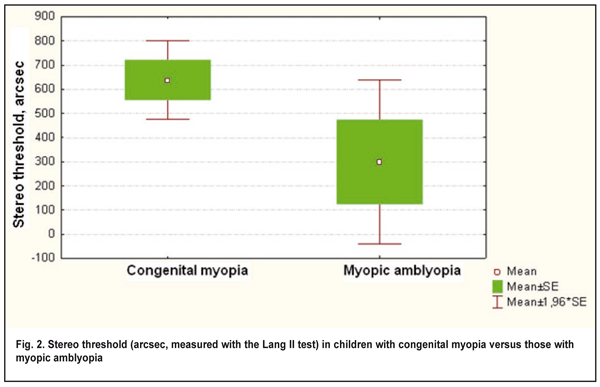
The length of time till the occurrence of a stereo effect in 84.2% of children was less than 20 s. The stereo threshold (Lang II random-dot test) of 400 to 600 arcsec, and the time till the occurrence of stereo effect of less than 20 s were found only in 28.5% (?2 =10.7, p=0.001) and 16.6%, (?2 =5.05, p=0.02), respectively, of myopic amblyopes. The stereo threshold (Titmus contour tests) was ? 100 arcsec in 42.6% of children with amblyopia. The average stereo threshold (Lang II random-dot test) in children with congenital myopia and in those with amblyopia was 638.4±74 arcsec and 300±123 arcsec, respectively (p > 0.05) (Fig. 2).
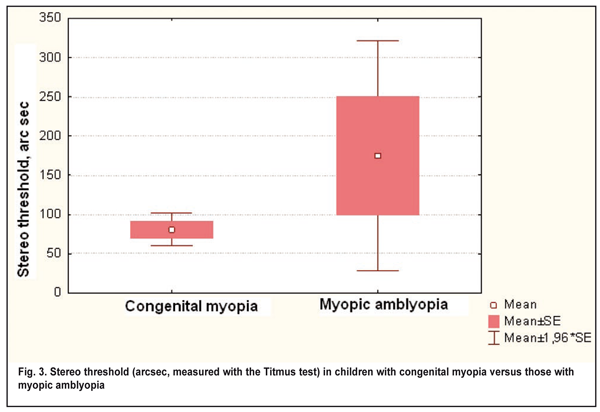
The average stereo threshold (Titmus contour tests) in children with congenital myopia was lower than in those with amblyopia (80.5±11.8 arcsec versus 175±75 arcsec), and the difference was statistically significant (p = 0.02) (Fig. 3).
Therefore, there was a difference in stereo thresholds between contour and random-dot tests for measurements in children with myopic amblyopia and in those with congenital myopia. Stereo thresholds obtained with Titmus test were higher in the former children than in the latter children (Fig. 3), and the difference was significant (p = 0.02). Most (85.4%) children with congenital myopia and only 28.5% of children with myopic amblyopia had a stereo threshold of 400 to 600 arcsec measured with the Lang test (p = 0.001). The length of time from presentation of a test object to the reaction of the individual was significantly shorter in congenital myopia (p = 0.02). It might be believed that in myopic amblyopia, a slower binocular information processing rate is observed, with perception of contour images reduced more substantially than that of random-dot stereograms. Conclusions First, stereovision was better in children with congenital myopia than in those with myopic amblyopia, which was evidenced by lower stereo thresholds obtained with Titmus test and Lang II random-dot stereotest. Second, contour and random-dot stereotests found that children with congenital myopia had better stereovision than those with myopic amblyopia, with low thresholds of less than 100 arcsec found in as much as 68.9% (Titmus Animals) and 80.7% (Titmus Circles). In addition, with Lang II random-dot stereotest, a stereo threshold of 400 to 600 arcsec was found in 88.46% of the former children compared to 28.5% of the latter children (p = 0.001).
Finally, a length of time (from presentation of a test object to the occurrence of a stereo effect) of less than 20 s was found in 88.46% of children with congenital myopia, and in 16.6% of those with myopic amblyopia. References
|